In March 2026, Andrej Karpathy quietly published an interactive dashboard that may turn out to be the most consequential piece of careers writing of the year.
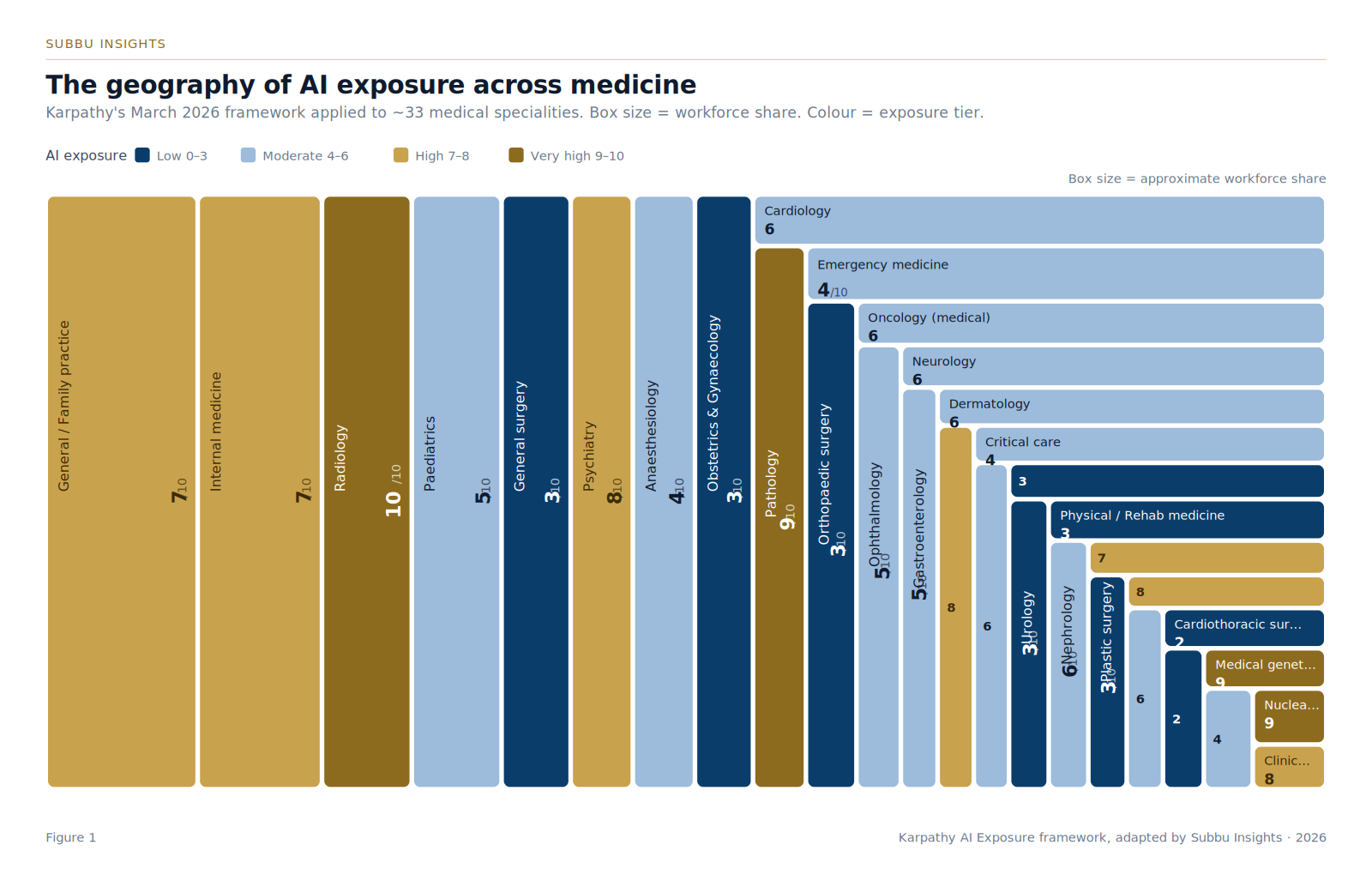
It scored 342 occupations on a single question — how much of this work could AI realistically perform? — and laid them out as a treemap, each tile sized by the number of people it employs. The finding was uncomfortable for the cognitive elite. Lawyers, accountants, financial analysts, software developers, paralegals, market researchers — the prestigious knowledge-economy jobs of the last forty years — clustered at 8 to 10 out of 10. Bartenders, roofers, ironworkers, and nursing assistants sat at 1 to 2.
Doctors landed in the middle. For procedural specialities — anaesthesiology, surgery, emergency medicine, critical care — the score was reassuringly low. Anaesthesia: 4. Surgery: 3. The reflexive medical response was predictable: we are safe.
That reading is partly true and dangerously incomplete.
01The Karpathy rubric, simply stated
Karpathy’s framework reduces to one question. Can the work product be produced from a laptop, away from the patient, away from the workshop, away from the room? If yes, the score climbs. If no, it falls.
Radiology scores 10 because the work is image interpretation rendered onto a screen. Construction scores 1 because the work is two people lifting a beam into place. Anaesthesia scores 4 because, fundamentally, you cannot intubate from your kitchen.
That is true. It is also the wrong unit of analysis.
02The decomposition trap
A speciality is not a single task. It is a portfolio of tasks bundled under a job title.
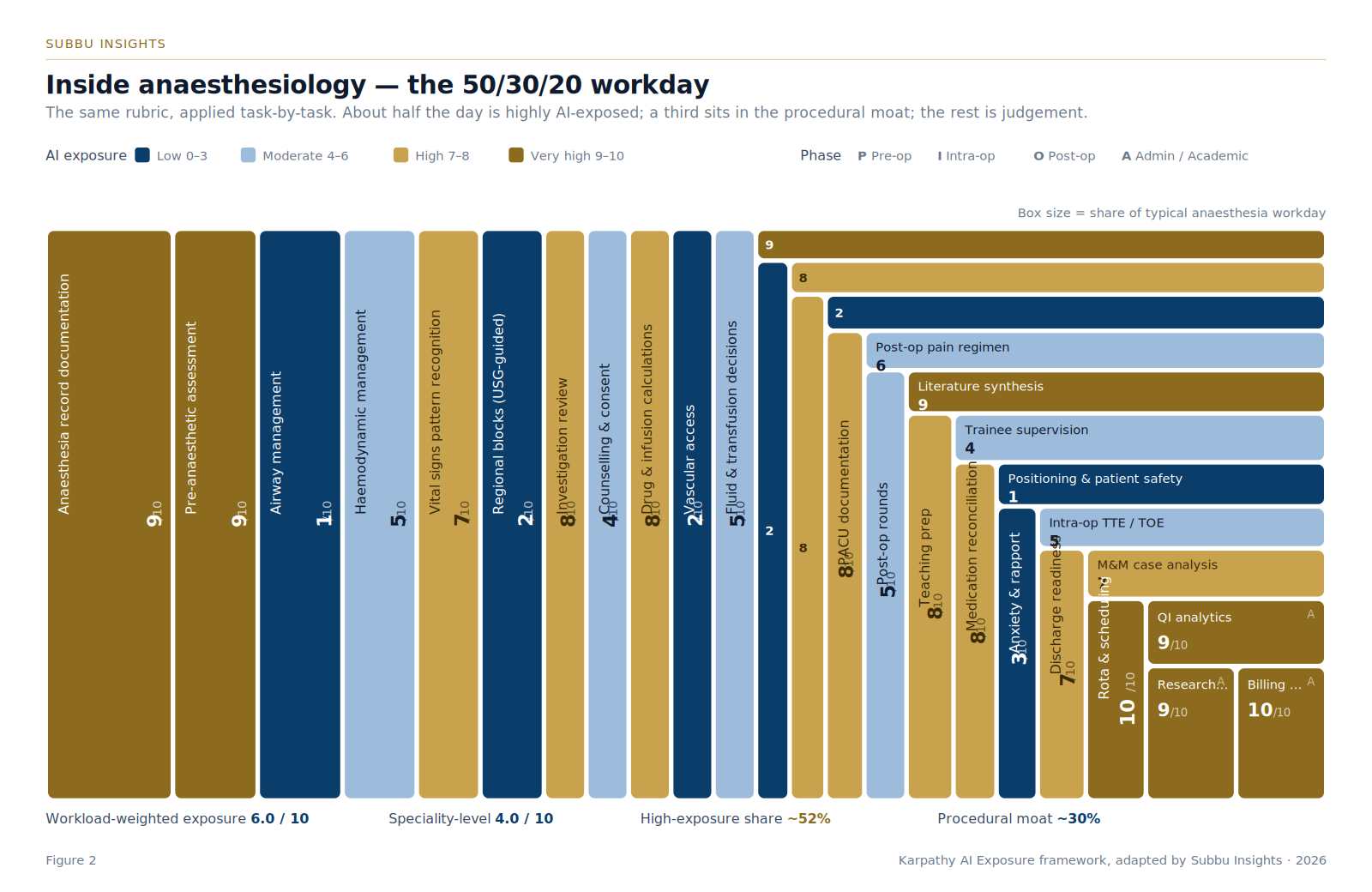
Apply Karpathy’s rubric to what an anaesthesiologist actually does across a working day — not “anaesthesiology” as an abstraction, but the concrete acts that fill the hours — and the picture changes.
The pre-anaesthetic assessment, the medication reconciliation, the risk stratification scores, the investigation review: all highly exposed. The intra-operative anaesthesia record, the drug dose calculations, the TCI pharmacokinetic modelling, the EEG/BIS interpretation, the vital-signs pattern recognition: highly exposed. The PACU documentation, the discharge-readiness assessment, the post-operative pain regimen: highly exposed. The literature synthesis for the M&M, the departmental rota, the QI dashboards, the billing: very highly exposed.
Then the procedural core — airway management, regional blocks, vascular access, crisis leadership. These score 1 to 2. Irreducibly human, for the foreseeable future.
When you weight each task by the share of the workday it occupies, the workload-weighted exposure score for anaesthesia is not 4 out of 10. It is approximately 6.
The same speciality, two honest numbers, depending on the unit of analysis. Both are valid. Only one is operationally useful.
03Three zones, one map
Roughly 52% of an anaesthesiologist’s workday sits in tasks scoring 7 or higher on AI exposure. This is the AI dividend — work that mature or near-mature AI can take 30 to 70% off our hands within twelve to twenty-four months. Documentation, prediction, scheduling, evidence synthesis, image and waveform pattern recognition.
Roughly 30% sits in the procedural moat — work that becomes more valuable, not less, as the cognitive layer commoditises. Airway, regional anaesthesia, vascular access, crisis leadership. The skill premium here will rise, not fall.
The remainder is the judgement layer — haemodynamic decisions, fluid management, post-operative pain — where the right model is neither replacement nor protection but augmentation. The AI suggests, the human decides, the system learns from the override patterns.
High-exposure cognitive work. AI takes 30–70% off our hands in 12–24 months.
Hands and voice. The skill premium rises as the cognitive layer commoditises.
Augmentation, not replacement. AI suggests, the clinician decides, the system learns.
That three-zone map is, I believe, the truest description of medicine in the AI era for any procedural speciality.
04The three layers around every clinical act
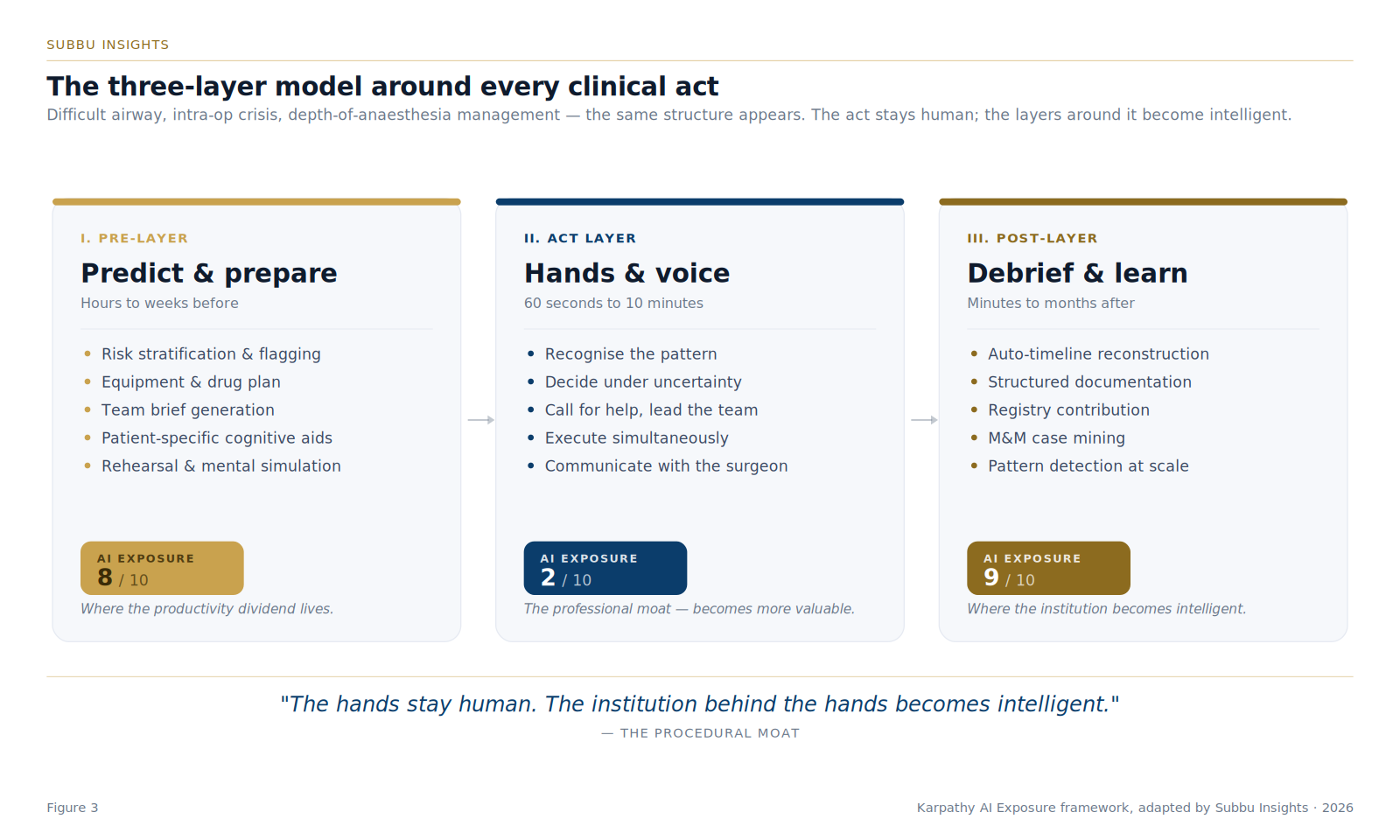
Take any high-stakes anaesthetic moment — a difficult airway, an intra-operative crisis, the management of depth on a TCI infusion — and you find the same structure.
A pre-layer where prediction and preparation happen. Highly AI-exposable. Risk scores, equipment plans, team briefs, mental rehearsal scaffolds. This is where the productivity dividend lives.
An act layer where the hands and the voice carry the work. Largely AI-proof. Laryngoscopy, the regional block, the chest compression, the team leadership in a code. This is the professional moat.
A post-layer where debrief and learning happen. Highly AI-exposable. Auto-documentation, registry contribution, M&M case mining, pattern detection across hundreds of cases. This is where the institution becomes more intelligent over time.
Anaesthesiologists who understand this geography will spend the next decade compounding capability. Those who do not will be doing the same work, less efficiently, in a profession that has quietly moved on.
05The augmented anaesthesiologist
The framing that resists both the hype and the denial is simple. AI does not replace the anaesthesiologist. It removes the cognitive friction around what the anaesthesiologist does best. Hands on the laryngoscope become more skilled, more deliberate, better resourced — because the preparation was sharper, the prior alerts were visible, the brief was clearer, and every prior event in the institution has been mined for what it can teach.
The unit of analysis that matters is no longer the algorithm, and not even the doctor. It is the system that holds them both — what I have come to call, with intent, clinical intelligence.
“The hands stay human. The institution behind the hands becomes intelligent.”
06The takeaway
Headlines about AI in medicine are mostly arguments about who is safe. That is the wrong question.
The right question is which 50% of your day you intend to keep, and which 50% you intend to hand to a system that can compound learning across thousands of patients in ways no individual ever can.
That, more than any single algorithm, is the real shape of medicine in the next ten years.
Dr Subramanyam S. Mahankali is Director of Anaesthesia at KIMS Hospitals — Ecity and Mahadevapura, Bengaluru. He writes on perioperative intelligence, AI in healthcare, and the future of anaesthesia at Subbu Insights.
Notes & References
- Karpathy A. AI Exposure Dashboard. Published March 2026. Interactive tool scoring 342 U.S. occupations on a 0–10 scale of how much of each job’s tasks AI can realistically perform. Dataset, methodology, and underlying scoring prompt published openly on GitHub.
- Karpathy A. Remarks at Sequoia AI Ascent 2026: “You can outsource thinking. You cannot outsource understanding.” The line that frames much of the analysis in this piece.
- Interactive lookup tool built on the Karpathy dataset, allowing job-title-level retrieval of AI exposure scores. Available as a Claude artifact at claude.ai/public/artifacts/aff3e505-8b48-4f35-99b9-c0276f4c1962.
- Workforce-share and workload-share estimates used to size the figures in this piece are illustrative, drawn from publicly available physician-workforce data and a reasoned task-time decomposition of a typical anaesthesia working day. They are intended to convey relative magnitude rather than precise enumeration, and will be refined in subsequent pieces of the series as institutional data becomes available.